科技之徒
场



正文
Abnormalities of the Arterial Pulse Wave in Young Diabetic Subjects
By HENRY LAX, M.D., AND ARTHUR W. FEINBERG, M.D.
With the technical assistance of William Urban
Abnormalities have been noted in the arterial pulse wave of human subjects with peripheral arteriosclerosis and with hypertension. The major change, diminution to disappearance of the dicrotic wave, has also been found in young diabetic subjects. The present study reports on the differences in the configuration of the arterial pulse wave of 162 diabetic subjects between the ages of 11 and 29 years and a comparable group of 275 nondiabetic controls. The findings seem to support the concept that the vascular abnormalities seen in diabetes mellitus are an integral part and not a complication of the disease.
THE increased tendency of the diabetic patient to develop evidences of vascular degeneration has been well documented. White,' Dolger,2 and others3' 4 have shown that almost all diabetic subjects have clinically apparent vascular lesions by the time they have had the disease for 15 years. The work of Mendlowitz and associates5 and of Megibow et al.6 with young adult diabetic persons suggests that there may be vascular impairment in this disease before such changes can be recognized clinically. Ditzel and Sagild7' 8 have described abnormalities of the capillaries of the bulbar conjunctiva in diabetic subjects as young as 4 years of age and in a few nondiabetic adults with a positive family history of the disease. To our knowledge, there have been no other reports of vascular impairment in diabetic children.
Previous studies9 have shown abnormal configurations of the arterial pulse wave in a high proportion of diabetic adults. This report is a comparison between the appearance of the arterial pulse wave in diabetic children and young adults up to the age of 30 years and in a comparable group of nondiabetic controls.
METHODS AND MATERIALS
A new recording technic has been utilized to obtain accurate, reproducible tracings of the arterial pulse wave without resorting to intra-arterial puncture. The method involves the application of a sensitive rubber cuff with an inelastic backing about the finger to be tested. Arterial pulsations are picked up from the digit and transinitted by a system of tubing to a piezo-electric crystal. The pressure changes in the cuff, due to arterial pulsations, are transformed into changes in electrical potential, which are then amplified, actuate a string type mirror galvanometer, and are recorded photographically.9' 10
The technic has been shown to be sensitive and to give reproducible results. The accuracy of the recordings has been demonstrated by the similarity of simultaneous intraarterial and periarterial tracings.9
Figures 1 and 2 show typical examples of normal and abnormal pulse waves as recorded by this technic. The change in the abnormal cases appears to be diminution to disappearance of the dicrotic wave. This change in the configuration of the dicrotic wave has previously been found in patients with arteriosclerosis, with hypertension, and in all adult diabetic patients over the age of 40 years.9


One hundred and sixty-two diabetic patients between the ages of 11 and 29 years were examined at either the Vanderbilt Clinic of the Columnbia-Presbyterian Medical Center or Camp NYDA, a summer camp for diabetic children sponsored by the New York Diabetic Association. All of these patients took insulin. None exhibited any evidence of arteriosclerosis or hypertension on careful physical examinations. Chest x-rays were normal, as was palpation of the peripheral blood vessels. Retinal vessels were examined independently by a group of ophthalmologists and adjudged normal.
Two hundred and seventy-five presumably normal control subjects between the ages of 11 and 29 years were also examined with this technic. Most of the children between 11 and 16 years of age were at the Pleasantville Cottage Camp for Children just outside New York City. None of the control subjects exhibited glycosuria and those with a family history of diabetes were not included in this section of the study.
RESULTS
Ninety-nine (62 per cent) of the 162 diabetic subjects had abnormal arterial pulse waves, as shown by a diminution to disappearance of the dicrotic wave. In contrast, only 22 (8 per cent) of the 275 presumably healthy young people, also between the ages of 11 and 29 years, had abnormalities of their arterial pulse wave recordings.
Subdivision of the diabetic and control groups by age did not alter the results (fig. 3). There were 203 normal children between the ages of 11 and 20 of whom only 7 percent displayed any abnormalities, whereas 60 per cent of 134 diabetic children of comparable age had diminished to absent dicrotic waves. There were 72 normal subjects between the ages of 21 and 30 years, of whom only 11 per cent showed any abnormalities while 68 per cent of 28 diabetic subjects in this decade had abnormal arterial pulse waves.

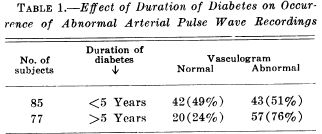
No correlation could be established between the severity of the diabetes, as measured by insulin requirements, and the presence of an abnormal arterial pulse tracing. The longer the duration of diabetes, however, the more likely was the pulse wave to be abnormal (table 1). About half of 85 subjects who had been diabetic less than 5 years had abnormal arterial pulse waves. Seventy-six per cent, however, were abnormal among 77 persons who had been diabetic longer than 5 years. None of these patients, it is important to emphasize, had any clinical evidence of vascular disease.
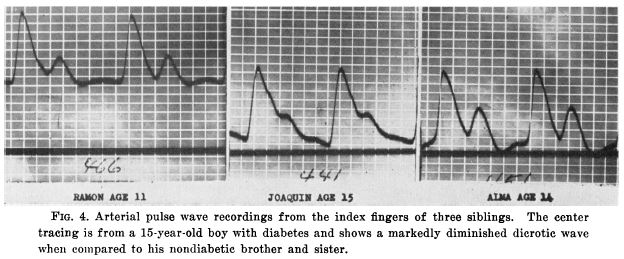
In some cases more than one child from the same family was studied. Figure 4 reproduces the recordings from the index fingers of 3 siblings, ages 11, 14, and 15. The tracing with the diminished dicrotic waves is that of a 15-year-old boy who had known diabetes for 6 years. Neither of his siblings is diabetic and both have well-defined dicrotic waves.
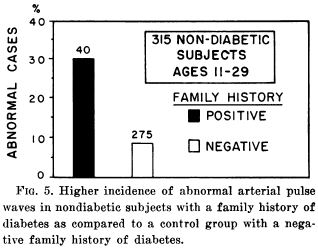
Forty normal subjects between 11 and 29 years of age, who gave a positive family history of diabetes, were also studied. Although none showed evidence of vascular disease, 30 per cent had abnormal arterial pulse wave recordings as compared to 8 percent abnormalities among 275 control subjects without a positive family history of diabetes (fig. 5.). Glucose tolerance tests were not performed.
DISCUSSION
The high incidence of arteriosclerotic changes in patients with diabetes mellitus is well known and, until recently, has been considered to be a complication of the carbohydrate derangements in the disease. Dolger2 first suggested that the circulatory and metabolic aspects may well be independent of one another and that vascular impairment may be a basic manifestation rather than a complication of diabetes. Support for this newer concept has been reported in the past few years. Mendlowitz5 performed calorimetric studies and demonstrated decreased digital blood flow in the toes of young diabetic adults that was independent of the severity, duration, or age of onset of their disease. Megibow6 reported evidences of peripheral vascular impairment in adult diabetic subjects, who had no clinical evidence of arteriosclerosis, by employing a microplethysmographic technic. Wagener"l has reported retinopathy in patients whose only manifestation of diabetes was a positive glucose tolerance test. Ditzel and Sagild7' 8 have demonstrated changes in the capillaries and venules of the bulbar conjunctiva of normotensive diabetic subjects as young as 4 years of age, none of whom showed any other evidence of vascular disease. They also reported that of 6 supposedly nondiabetic adults who showed marked abnormalities of their capillaries, 4 had diabetes in their immediate family history.
Our results lend additional support to the concept that diabetes mellitus is, in actuality, a multifaceted disease process. The pulse wave alterations are present early in the course of the disease and, are already found in half of the children studied when diabetes had been present less than 5 years. An even higher proportion of abnormal cases is found as the duration of the disease lengthens. No correlation could be established between the presence of this abnormality and the severity of the diabetes, as measured by insulin requirements. It is important to emphasize that all of these patients had severe enough diabetes to require insulin. None had any clinical stigmata of vascular disease.
Further evidence that the vascular abnormalities are not a consequence of the disturbed carbohydrate metabolism is the fact that a high percentage of normal children with a positive family history of diabetes show alterations of their arterial pulse waves. Thirty per cent of the patients with a positive family history had abnormal dicrotic waves as compared to only 8 per cent abnormalities in the control group.
A major drawback to clinical studies in this field has been the lack of simple methods of examining the vascular system. Physical examination rarely shows evidence of vascular abnormalities in diabetic children. Microplethysmographie and calorimetric examinations require careful controls of room and extremity temperature and are impractical for large-scale studies. The technic described here has the advantage of being simple to use and of giving accurate, reproducible recordings of the arterial pulse wave without requiring intra-arterial puncture.
The mechanism of the observed change in the dicrotic wave is still not clear. Classically, the dicrotic wave has been ascribed to rebound against the closed aortic valve. More recent studies12' 13 have indicated that peripheral factors play an important role in the formation of the dicrotic segment of the arterial pulse wave. Our recent study10 of the different effects produced by epinephrine and norepinephrine on the dicrotic wave, further supports the concept that the dicrotic wave is predominantly of peripheral origin.
Whether the altered dicrotic wave found in young diabetic patients reflects some change in elasticity or whether it represents true organic change in the blood vessels of these people is undetermined. Whatever the cause, a method has been presented that seems to offer a means of detecting changes in the configuration of the arterial pulse wave of young diabetic patients, and in some nondiabetic subjects with a family history of the disease, that antedates clinical evidences of change in their vascular system.
SUMMARY
A simple, accurate reproducible technic for recording the arterial pulse wave without requiring intra-arterial puncture has been used to study 162 diabetic subjects between the ages of 11 and 29 years and a similar group of 275 nondiabetic controls. Sixty-two per cent of the 162 diabetic subjects had abnormal arterial pulse waves. The change noted was diminution to disappearance of the dicrotic wave. None had any clinical evidences of vascular disease. Only 8 percent of 275 nondiabetic control subjects of the same age group had abnormal configurations of the arterial pulse wave.
Forty-nine per cent of the diabetic patients who had the disease less than 5 years had abnormal pulse waves; 76 per cent were abnormal in the group who had been diabetic longer than 5 years. Although apparently nondiabetic themselves, 30 per cent of 40 patients with a positive family history of diabetes had abnormal arterial pulse waves.
These findings seem to support the concept that the vascular abnormalities seen in diabetes mellitus are an integral part and not a complication of the disease.
ACKNOWLEDGMENT
We would like to express our appreciation to the New York Diabetes Association and to the Director and staff of Camp NYDA and of the Pleasantville Cottage Camp for Children for their whole-hearted cooperation in every phase of this study.
REFERENCES
1. WHITE, P., AND WASKow, E.: Arteriosclerosis in childhood diabetes. Proc. Am. Diabetes
Assoc. 8: 139, 1948.
2. DOLGER, H.: Clinical evaluation of vascular damage in diabetes mellitus. J.A.M.A. 134: 1289, 1947.
3. DRY, T. J., AND HINEs, E. A., JR.: The role of diabetes in the development of degenerative vascular disease. Ann. Int. Med. 14: 1893, 1941.
4. BARACH, J. H.: Arteriosclerosis and diabetes. Am. J. Med. 7: 617, 1949.
5. MENDLOWITZ, M., GROSSMAN, E. B., AND ALPERT, S.: Decreased hallucal circulation, an early manifestation of vascular disease in diabetes mellitus. Am. J. Med. 15: 316, 1953.
6. MEGIBOW, R. S., MEGIBOW, S. J., POLLACK, H., BOOKMAN, J. J., AND OSSERMAN, K.: The mechanism of accelerated peripheral vascular sclerosis in diabetes mellitus. Am. J. Med. 15: 322, 1953.
7. DITZEL, J., AND SAGILD, U.: Morphologic and hemodynamic changes in smaller blood vessels in diabetes mellitus. II. Degenerative and hemodynamic changes in bulbar conjunctiva. New England J. Med. 250: 587, 1954.
8. -: Angioscopic changes in the smaller blood vessels in diabetes mellitus and their relationship to aging. Circulation 14: 386, 1956.
9. LAX, H., FEINBERG, A. W., AND COHEN, B. M.: Studies of the arterial pulse wave. I. The normal pulse wave and its modification in the presence of human arteriosclerosis. J. Chron. Dis. 3: 618, 1956.
1.0. FEINBERG, A. W., AND LAX, H.: Studies of the arterial pulse wave. Circulation 16: 1125, 1958.
11. WAGENER, H. P.: Retinopathy in diabetes mellitus. Proc. Am. Diabetes A. 5: 203, 1945.
12. HAMILTON, W. F., AND Dow, P.: The patterns of the arterial pressure pulse. Am. J. Physiol. 141: 235, 1944.
13. ALEXANDER, R. S.: Factors determining the contour of pressure pulses recorded from the aorta. Fed. Proc. 2: 738, 1952.

评论
目前还没有任何评论
登录后才可评论.